This last day of “NERVEmber ® and Art Every Day Month (AEDM) is about adaptability, solutions, and coping targeted at post-survival Thriving with arachnoiditis and its numerous consequential conditions.
The Arachnoiditis Apocalypse is accompanied by MANY lessons that are as diverse as the people living with it. My life was permanently altered in many ways. It took time to grieve what was gone and to realize, “altered” is not the same as destroyed.
Much of the content I post is designed to offer search terms you may not have considered and to let you know what has or has NOT worked for me. What I share is based on my own experience and is NOT ever intended as medical advice or treatment for you. Always be sure to consult your trusted practitioners prior to making any changes to your treatment plan.
The Bullet Points ~(This is NOT a to do list.)
Own your Wellness.
Go Gently and Listen to Your Body.
Celebrate Little Things. Grace lives in them.
Know your triggers. Navigate your pain.
(For Adhesive Arachnoiditis) Assess the impact of any obstruction to natural cerebrospinal flow. Find out which positions mitigate the blockage to restore as much optimum flow as safely as possible. (Whether it is a leak or a blockage, frequent spinal or positional headaches may be an indicator of a disruption of the natural flow of spinal fluid.)
Pace yourself, but KEEP moving.
Get Creative – The Creative Process Heals
Be Mindful. Intentional use of time minimizes the perception of lost time.
Be Informed. Not obsessed.
“Escape” in moderation.
Connect with Others. Solitude is Beneficial. Isolation is Lonely. Loneliness is destructive. Healthy connections create harmony in mind, body, and spirit.
Work with a trusted practitioner to document your progress and learn which treatment and support are right for you.
DETAILS
Adaptability is the foundation for Thriving with Arachnoiditis.
The significance of Cerebrospinal Fluid Flow Rotation was the key that unlocked the mystery of how I could re-learn to live my life. In my case, this obstruction at multiple spinal levels IS, and will always be, the origin of much of my neurological dysfunction. It became such a big part of pain navigation that a pervasive awareness of it underlies everything I am doing now. Sometimes, quietly tracking my remaining minutes, I am conscious of it running out like the sand in the hour glass shown in the art journal doodle above.
Though at first I didn’t know how to differentiate these factors from the others, I did learn. For me, maximum vertical time was approximately two and a half hours before symptoms of CSF entrapment/blockage would begin to impair my ability to function. However, IF I made sure to get horizontal every two hours, even when I was feeling okay-enough in the moment, eventually I had the power to minimize the impact of those symptoms. As is common for arachnoiditis survivors, invasive procedures are contra-indicated in my care. This obstructive scar tissue cannot be removed. (These symptoms have some similarities to those of a CSF leak. The difference is there is NOT a leak. The fluid is still in there trapped in the wrong place in the spinal canal. It puts pressure in those places while the brain is essentially deprived of an adequate amount.)
Eight years into Arachnoiditis Survival, I developed Complex Regional Pain Syndrome (CRPS). Though I wouldn’t wish it on anyone, my biggest lesson came in learning more about how to manage it. As I changed my habits to reduce inflammation, I inadvertently discovered that, over time, I was reducing the swelling in my spinal cord. Eventually, there was more room for the spinal fluid to flow around the scar tissue. In 2019, twelve years after leaving the workforce due to unemployability, I was able to return to working in the local community. From 2019 to 2023, I continued practicing all that I had learned to navigate and adapt to this injury.
A year ago today, I fell down some icy stairs and broke a bone in my back. Ordinarily this should have taken about twelve weeks to heal. It didn’t. Complicated by what was most-likely a bone marrow infection and the discovery of an undetected compression fracture at a different spinal level resulting in a new impact-trauma-induced arachnoiditis flare, 2024 has been a very long year.
So, this NERVEmber, now that I finally have all the details about what I am dealing with this time, I am revisiting all of the lessons I learned along the way to this moment.
“NERVEmber ® brings awareness to conditions that have nerve pain as a symptom. The International Pain Foundation hosts the OFFICIAL NERVEmber project events each year. Since its inception, tens of thousands of nerve pain patients and organizations have signed on to help promote NERVEmber.“
Just a few minutes ago, it dawned on me that putting these here may be more useful than posting them where I had been putting them. So, here are some social media posts I’ve shared these last few weeks about the Nerve Pain Conditions which have had an impact on my life. There is a lot of info in this post. Pace yourself.
A known consequential condition of spinal adhesive arachnoiditis, “Complex Regional Pain Syndrome (CRPS) can affect the bone marrow, leading to bone thinning or excess bone growth. In rare cases, the bones may become rough or enlarged. CRPS is a painful disease that occurs when the sympathetic nervous system goes awry. It can cause a variety of symptoms, including: Pain Swelling Redness Temperature changes Hypersensitivity, especially to cold and touch Muscle spasms and tightening CRPS can also cause the affected limb to become cold and pale. Over time, the condition can become irreversible. In some cases it can spread to other areas of the body. CRPS is sometimes associated with bone marrow edema syndrome (BMES). Complex regional pain syndrome (CRPS) has been known by many other names, including: Reflex sympathetic dystrophy syndrome (RSDS) Algodystrophy Causalgia Transient osteoporosis Post-traumatic dystrophy Reflex neurovascular dystrophy The International Association for the Study of Pain (IASP) introduced the term CRPS in 1994 to describe a variety of post-traumatic neuropathic pain conditions in the limbs. However, the name change from RSDS to CRPS has not been universally accepted.
“Listen-whatever it is that makes you wake up, whatever it is that makes you feel a moment of peace or a glimmer of hope, just keep it close. Please, live for it. Make sure that you focus on it. Make sure that you make time for it. I don’t care what it is. You have to understand that happiness does not have to be this big all-consuming thing. Sometimes happiness is your morning cup of coffee. Sometimes it is the smell in the street after it rains, or your favorite song played on repeat for three hours straight. Sometimes happiness is your friend’s laughter or the way the sky looks through the trees in your favorite park. If it keeps you going, if it ignited something within you, it doesn’t matter how small or grand it is. Just hold on to it. Let it save you.” ~Bianca Sparacino
Art is that for me.
Nervember Post – Gratitude 11.28.2024
Back to the drawing board. Though 2023 was a fantastic year of wellness and possibilities, 2024, blessed with moments of Grace between challenging days has been long and pushes me to tap into lessons learned and to seek new wisdom to heal more stuff… … Again. Future Art Offerings will be coming to patrons from the Ostrich Cot. …………………………………………………………………………… Throwback-but-Thankful Thursday: To understand my Gratitude around the discovery and support I received from the #OstrichCot you can Click Through to see portrait examples from Ten Years Ago here: https://www.youtube.com/watch?v=VQYG6s6LBR0 P.S. These are portraits in progress from the Arachnoiditis Survivor Portrait Project. New Portrait Order Options Are Not Available at this time.
Nervember Post 11.26.2024 Spinal Arachnoiditis and CSF Flow Blockage
A preventable permanent spinal cord injury, “Chronic adhesive spinal arachnoiditis (SA) is a complex disease process that results in spinal cord tethering, CSF flow blockage, intradural adhesions, spinal cord edema, and sometimes syringomyelia. Mechanism: When the CSF cannot circulate freely, it can build up pressure within the spinal cord, causing fluid-filled cavities to form. Symptoms: Symptoms can vary depending on the location and size of the obstruction but may include pain, weakness, numbness, muscle atrophy, spinal headaches, and impaired coordination in the affected areas of the body.” Prevention is the only cure. https://www.medicinenet.com/is_there_a_cure_for_adhesive_arachnoiditis/article.htm Image| Axial View of Thoracic Spine MRI post off-label use of spinal anesthesia containing 5% lidocaine with epinephrine. See also: “Potential Neurotoxicity of Spinal Anesthesia with Lidocaine” Michael E. Johnson MD, PhD https://www.mayoclinicproceedings.org/article/S0025-6196(11)64644-2/fulltext
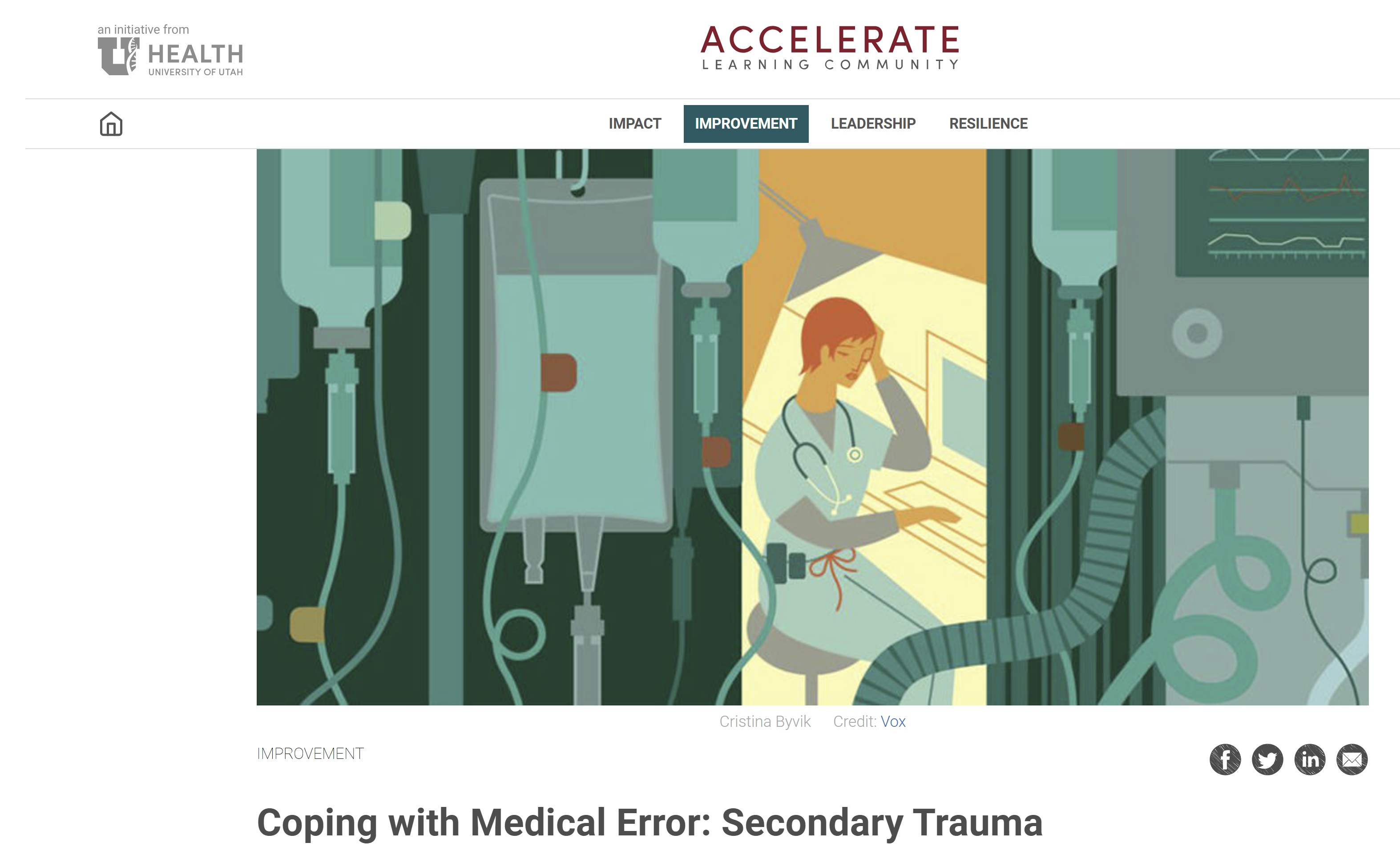
NERVEmber Post 11.22.2024 MEDICAL TRAUMA (Image credits to sources as noted)
“We don’t talk about medical trauma all that often. But for many, trauma at the hands of healthcare professionals is real — and knowing how to heal matters.“ https://psychcentral.com/ptsd/medical-trauma #MedicalHarmSurvivors #TraumaInformedCare #DoNoHarm ” Around 1 in every 10 patients is harmed in health care and more than 3 million deaths occur annually due to unsafe care.” https://www.who.int/news-room/fact-sheets/detail/patient-safety
“Medical trauma is a form of psychological trauma resulting from medical diagnosis or intervention. The resulting symptoms can include post traumatic stress disorder (PTSD), depression, anxiety, and disrupted sleep. Through acknowledgement and acceptance — and with the proper treatment from a mental healthcare professional — most people can manage their symptoms and experience full recovery from this kind of trauma.“ https://www.choosingtherapy.com/medical-trauma/ Medical Trauma: How to Cope When Treatment Hurt You https://hartzellcounseling.com/medical-trauma-how-to-cope-when-treatment-hurt-you/
Medical visits can significantly trigger trauma for survivors of patient harm, as the healthcare environment can re-traumatize them by reminding them of previous negative experiences, particularly when elements like invasive procedures, loss of control, or power imbalances are present, causing anxiety, fear, and flashbacks.
Trauma-informed care: Healthcare providers should be trained in trauma-informed care practices, which involve understanding how trauma can impact patients and taking steps to create a safe and supportive environment. Open communication: Allowing patients to share their experiences with past medical trauma and openly discussing concerns before any procedures. Patient autonomy: Providing patients with choices and control over their care whenever possible. Respectful approach: Using empathetic language, validating patients’ feelings, and avoiding unnecessary touch or pressure. Collaboration with mental health professionals: If needed, involving mental health professionals to support patients through difficult medical encounters.
Chronic Pain and PTSD Sadie E. Larsen, PhD and Katherine E. Hadlandsmyth, PhD
When people experience both chronic pain and posttraumatic stress disorder (PTSD), each condition can exacerbate the other. This article provides information and options to providers working with people who have both PTSD and chronic pain. https://www.ptsd.va.gov/professional/treat/cooccurring/chronic_pain_guide.asp
“Medical trauma or medical post-traumatic stress disorder is painfully under-represented, yet overwhelmingly common.
What Is Medical PTSD? Simply put, medical PTSD is PTSD. Most, if not all, typical symptoms of PTSD are congruent with those of Medical PTSD. The only difference is in the traumatic event itself.
The Anesthesiologist who caused the spinal cord injury I survived was simply doing what he was taught following the guidelines for the Accepted Average Standard of Care in NYS. In my extensive experience as a patient, most practitioners have good intentions.
NERVEmber Post 11.21.2024 ~ Nerve Pain and The Anatomy of Sitting
“Prolonged sitting, especially on an unsupportive surface, can flatten the natural curves of our spine, placing undue stress on the vertebrae and surrounding tissues. The lumbar curve is especially at risk. When we slouch on a sofa, this curve diminishes, leading to a strain on the discs between the vertebrae. Over time, this can lead to discomfort, fatigue, and long-term health issues.” https://dantefurniture.co.uk/blogs/lifestyle-and-wellbeing/sofas-and-your-spine-the-connection-between-sitting-and-posture
“In this time where most people are currently still working from home, it can be tempting to stay on the sofa with your laptop all day. But, this is far worse and can do a lot more damage to your back and neck than sitting at a desk or a table. […] As most sofas have a deep seat, it can be tricky sitting upright in a comfortable way – especially if you have shorter legs. Add two or three cushions behind you to support your upper back to prevent from slumping. Supporting your upper back rather than your lower will help to keep your pelvis and your spine upright and your head will also be better balanced which will then reduce pressure on the lower back. Experiment with how many cushions you use to find your most comfortable position.” https://swyfthome.com/blogs/lifestyle/sit-on-a-sofa-to-avoid-back-pain Vagopathy “Vagopathy is the result of the “facedown lifestyle” looking at screens and phones all day, traumatic injury, hypermobility syndromes, and degenerative wear and tear. The subsequent neck instabilities these problems cause is “vagopathy” (the destruction of the vagus nerve). The resulting compression and altered signals of the vagus nerve can lead to a condition called sympathetic dominance. This is a situation where a person feels stressed all the time. This is more than phycological stress, this can be a structural stress.” https://caringmedical.com/prolotherapy-news/sleep/
NERVEmber Post 11.20.2024 ~ The Truth About Epidural Steroid Injections
This 2014 video gives a good demo, at the 00:30ish mark, of how spinal injections can have an impact on spinal nerves and discusses the balance between risks and benefits. https://www.youtube.com/watch?v=cPieVQdXP58 Always request that spinal injections be guided live by medical imaging, fluoroscopy, during the procedure. Cancel or Reschedule if this option is not available. When receiving spinal anesthesia, always confirm what anesthetic is being used and that is safe for spinal use. Check the adverse events listings to find out more about it before your procedure. The campaign to push this arachnoiditis awareness effort forward was partially inspired by the deaths and adverse outcomes of people who survived the 2012 nationwide fungal meningitis outbreak caused by epidural steroid injections. Designed to empower arachnoiditis survivors, The Survivor Portrait project was part of this awareness campaign after I was asked to tell my own story. Between 2014 and 2018 this project grew into an international creative wellness resource serving survivors in 93 countries. (WordPressReport 2015) https://sheilalynnkart.com/section/396432_Arachnoiditis_Survivor_A_Portrait_of.html
More About the fungal meningitis outbreak: “In 2012, a multistate outbreak of fungal meningitis occurred after patients received contaminated steroid injections from the New England Compounding Center (NECC) in Framingham, Massachusetts: Timeline: The first case was confirmed in Tennessee on September 18, 2012. By October 23, 2013, there were 751 patients and 64 deaths. Causes: The contaminated steroid was methylprednisolone acetate (MPA), which was preservative-free. The NECC used fictional and celebrity names on fake prescriptions to dispense the drugs. Response: The CDC, state and local health departments, and the FDA investigated the outbreak. Clinics and health departments contacted patients who received the contaminated injections and referred them for treatment. Sentences: More than a dozen people linked to the compounding pharmacy were convicted, including: Barry Cadden: Sentenced to nine years in prison in 2017, then resentenced to 14.5 years in 2021. In 2024, he was sentenced to 10 to 15 years in prison on Michigan state charges of manslaughter. Carla Conigliaro: Sentenced to one year of probation and a $4,500 fine. Douglas Conigliaro: Sentenced to two years of probation and a $55,000 fine. Gene Svirskiy: Sentenced to 30 months in prison and one year of supervised release. Christopher Leary: Sentenced to two years of probation and 100 hours of community service.” #ArachnoiditisSurvivor #ArachnoiditisAwareness
NERVEmber ~ A SITTING DISABILITY
EVERY CHAIR. EVERYWHERE. Having a sitting disability brings out interesting social observations. People get very antsy if you don’t sit down when they are seated. It’s rare to find an exception to this behavioral conditioning. During neurological flares, I have yet to find a chair that does not quickly feel like the one shown here. Trust me when I say, I have tried. If you see me sitting and I seem exceptionally distracted it is because there is likely an entirely secondary dialogue happening in my mind to talk myself out of the belief that I am being stabbed incessantly while I sit there. …AND wondering when this “flare” will be over… Hint: A person with a sitting disability caused by an injury to the sympathetic or autonomic nervous system may also be wearing many layers of clothing to buffer the impact and/or manage the intermittent bizarre hot and cold flashes that are part of this package. #CRPSawareness #SpinalArachnoiditisAwareness ………………………………………………….. “A “sitting disability” is the result of a medical condition causing severe pain when an individual is sitting. It is typically a symptom of an underlying condition, such as lower back pain, sciatic nerve pain, piriformis syndrome, or failed back surgery syndrome. It may also be related to fibromyalgia, myofascial pain syndrome, pudendal neuralgia, or coccydynia. The period of time sitting comfortably varies per individual.” “A sitting disability is a medical condition that makes it difficult or impossible to sit, usually due to pain. It can affect people with or without chronic standing issues, including those who use mobility aids. Sitting disabilities can be caused by a number of conditions, including: • Chronic back pain • Pain from the pelvis • Pain from nerves, ligaments, muscles, or fascia • Conditions related to the nervous system • Sciatic nerve pain • Piriformis syndrome • Failed back surgery syndrome • Fibromyalgia • Myofascial pain syndrome • Pudendal neuralgia Sitting disability is an umbrella term that groups people with a variety of medical conditions together based on their common consequences. These consequences can include: Difficulty fitting into the prevailing norms of a sitting society, Difficulty traveling, Difficulty retaining employment, and Feelings of distrust or inauthenticity.” https://www.painscale.com/article/what-is-a-sitting-disability #NERVEmber is Nerve Pain Awareness Month Though individual experiences vary greatly due to the diverse causes of sitting disability, additional support and information about life with a sitting disability can be found at: “I am vertical living with a sitting disability” https://overland.org.au/2021/07/i-am-vertical-living-with-a-sitting-disability/ “What happens when you can’t sit down.” https://myuprightlife.com/index.php/sitting-disabilities/health-conditions/ “Falling through the cracks; recognizing sitting disabilities.” https://www.tandfonline.com/doi/full/10.1080/09687599.2018.1545111 “I have a sitting disability. What that means.” https://www.christinairene.com/wp/archives/1914 Image| Found in the public domain on a traveling blog many years ago when I was writing about traveling as an arachnoiditis survivor doing portraits to empower other survivors. I’ve lost track of who posted it. If you know the source, please let me know so that I can post proper credit. Thanks!
NERVEmber ~ AEDM Post 11.18.2024 ~ “Why Be Happy When You Can Be Normal”
“I have noticed when all the lights are on, people tend to talk about what they are doing – their outer lives. Sitting round in candlelight or firelight, people start to talk about how they are feeling ~ their inner lives. They speak subjectively, they argue less, there are longer pauses. To sit alone without electric light is curiously creative. I have my best ideas at dawn or at nightfall, but not if I switch on the lights, then I start thinking about projects, demands, deadlines, and the shadows and shapes of the house become objects, not suggestions, things that need to be done, not a background to thought.“ ~Jeanette Winterson Author of Oranges Are Not The Only Fruit and Why Be Happy When You Can Be Normal https://www.jeanettewinterson.com/
NERVEmber and AEDM Post 11.15.2024 ~ “You don’t have to be pretty.”
Studio selfie 2022
“You don’t have to be pretty. You don’t owe prettiness to anyone. Not to your boyfriend/spouse/partner, not to your co-workers, especially not to random men on the street. You don’t owe it to your mother, you don’t owe it to your children, you don’t owe it to civilization in general. Prettiness is not a rent you pay for occupying a space marked ‘female.‘” – Erin McKean Flashback Friday – posted for Art Every Day Month 2015– “Human, Naturally” “Survival and recovery impact the individual sense of vanity. Be it the superficial cliche concept of “beauty” or a long-lived appreciation of our “inner beauty”, our self-image seldom escapes the experience unscathed. For all time but, especially, in modern culture; the pressure to conform to the concepts of beauty and grooming of the status quo is directly linked to our ability to be taken seriously by the influential populations of society.
Not only must Survivors overcome the physical limitations imposed upon them but, we must also find a balance within ourselves which allows us to reconcile the alterations in our physical appearance which result from that struggle. […] The reality is, that our appearance can condemn us to a marginal existence. Subconsciously, we fight against that. We think nothing of using the convenient products available to us to allow us to prevent that from happening.“ ~slk Read more about the social conditioning around the relationship between looking healthy and feeling healthy at artforarachnoiditis.org here: https://artforarachnoiditis.org/2015/11/13/art-every-day-month-day-13/ #NERVEmber #OpenlyGrey
NERVEmber and AEDM Post 11.15.2024 “Autumn Ice” and CRPSand Bones
When uncontrolled or “flaring” … Most commonly, CRPS presents with hot, red, swelling and burning pain when the nerves allow too much blood to enter the vessels. However, in some cases, like mine, it can also present as feeling perpetually cold with blueness in the skin, cold flashes and chills with cold pain similar to frost bite because the opposite occurs. The nerves don’t allow enough blood to enter the vessels. (Paraphrasing/over-simplifying this explanation as it was described to me years ago.) For many it includes the body’s inability to regulate temperature. Usually, I hurt before I know the temperature has dropped. Cold sends pain signals instead of thermal warning signs. Because: “The sympathetic nervous system plays a role in the chronic cold phase of complex regional pain syndrome (CRPS): Vasoconstriction During the chronic cold phase, α-adrenoreceptors become more sensitive to circulating catecholamines, which leads to vasoconstriction and decreased blood flow. Sympathetically mediated pain Adrenoreceptors on nociceptive fibers lead to sympatho-afferent coupling, which produces sympathetically mediated pain.
Other aspects of CRPS include: Allodynia: People with CRPS may experience sensations like warmth or cold as painful.
Neurogenic inflammation: The redness and swelling of CRPS may be different from normal swelling after an injury.
Hypoxia: Restricted blood flow reduces oxygen in tissues, which causes pain.
Bone abnormalities: CRPS is often associated with thinning or remodeling of bone, which can irritate nearby nerves.
Movement disorders: Many people with CRPS have impaired muscle strength and movement disorders.“ ………………………………. CRPS (Complex Regional Pain Syndrome) is a known consequential condition of spinal adhesive arachnoiditis. Arachnoiditis is a preventable spinal cord injury caused by the neurotoxins in spinal injections and invasive spinal procedures. Gastroparesis is known to be associated with both. ………………………………………… Art| “Autumn Ice” Tree Project in the Creative Wellness Garden sheilalynnkart.com
“When facing a chronic illness with no cure and no available treatment, the most important steps are to educate yourself about your condition, build a strong support system, prioritize self-care through healthy lifestyle choices, seek professional help from doctors and therapists, and explore potential management strategies to optimize your quality of life; this may involve managing symptoms, participating in clinical trials, and finding ways to adapt to limitations caused by the illness.“ #Nervember #CRPSAwareness #ArachnoiditisAwareness #MGUSPeripheralNeuropathyAwareness
SOCIAL MEDIA USE
NERVEmber Selfie for Social Media Profile Picture
Despite my longstanding struggle with over-use of social media, I believe it is a powerful tool that can be used to create healthy connections. “With great power comes great responsibility.” ~Stan Lee after Voltaire (maybe?) Side note: fact-checking is only as reliable as the sources providing the “facts”… Hence the current long season of doubt. ‘With Great Power Comes Great Responsibility’: From Age-Old Axiom to Spider-Man’s Mantra It all started with Jesus. Or Muhammad. Or the Reign of Terror. By Ellen Gutoskey |Mar 29, 2024 https://www.mentalfloss.com/posts/with-great-power-comes-great-responsibility-phrase-origins #DefyTheSpin #OwnTheChoices